LECTURES IN MAXILLO-FACIAL RADIOLOGY
Interpretation & Differential Diagnosis for Dental Students and Practitioners
(2 videos / 17 lectures)

Dr. Frederiksen earned his DDS degree from University of Minnesota and Ph.D (Radiation Biology) from SUNY at Buffalo, Buffalo, NY. He is formerly Professor and Director of Oral and Maxillofacial Radiology at Baylor College of Dentistry, TAMUS-HSC and founder of its Maxillofacial Imaging Center. He is a Diplomate and past President of the American Board of Oral and Maxillofacial Radiology.

Dr. Hui Liang earned her DDS degree and Ph.D (Prosthodontics) from Peking University School of Stomatology, P.R. China and her Master’s degree (Oral and Maxillofacial Radiology) from the University of North Carolina at Chapel Hill, NC. She is currently tenured professor in the Department of Diagnostic Sciences, Texas A&M University College of Dentistry. She is a Diplomate of the American Board of Oral and Maxillofacial Radiology and past Treasurer of the American Academy of Oral and Maxillofacial Radiology.
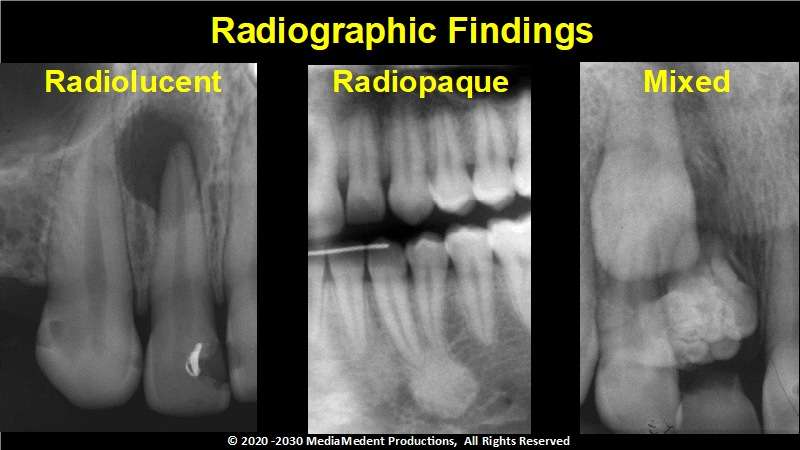
Lecture 1: The Introduction. One step in the formation of a differential diagnosis is to describe the lesion’s presentation, does it appear radiolucent, radiopaque, or does it have characteristics of both radiolucency and radiopacity? Video 1.
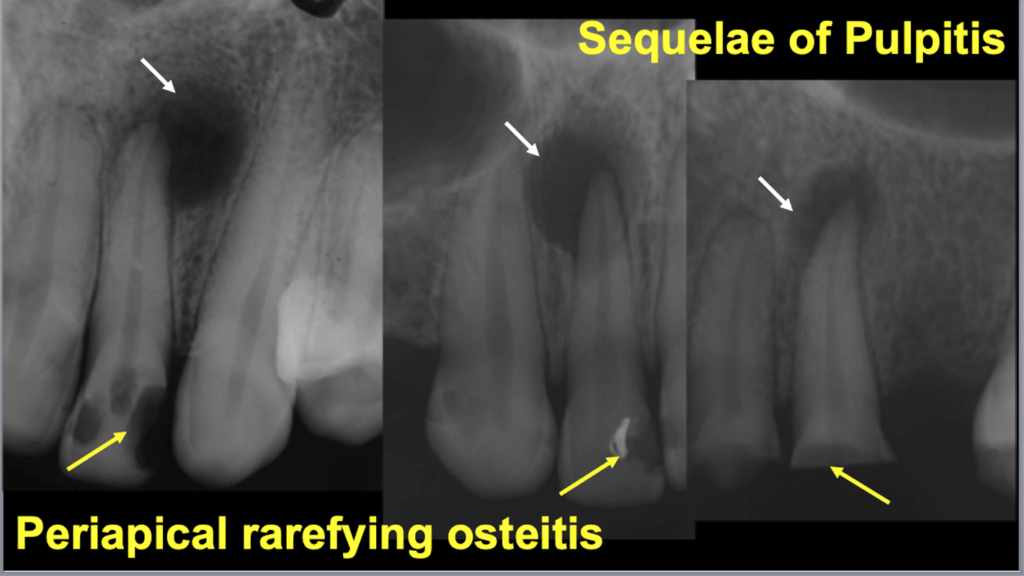
Lecture 2: Radiolucent Lesions Associated/Superimposed with Teeth. A radiolucency associated with the apex of a non-vital tooth represents the image of periapical rarefying osteitis. Video1.
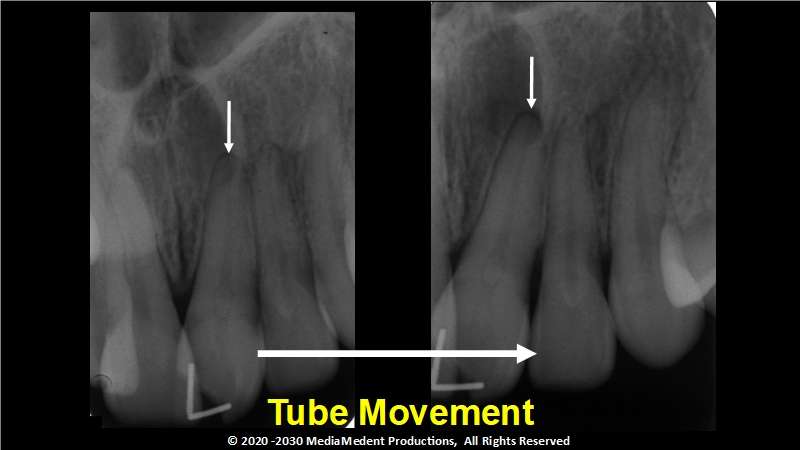
Lecture 3: : Radiolucent Lesions Not Associated with Teeth, Introduction. In this illustration, relative to the tooth’s apex the image of the lesion moved to your right as the X-ray tube was moved to the patient’s left. This allows you to locate the lesion to the lingual of the apex of the left central incisor. Video 1.
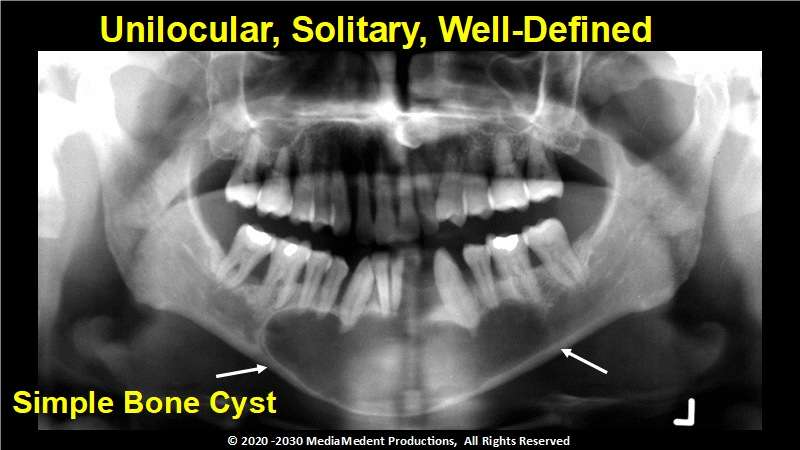
Lecture 4: Radiolucent Lesions Not Associated with Teeth, Unilocular, Solitary, and Well defined Radiolucencies. During the course of an examination a panoramic radiograph revealed a unilocular, solitary radiolucency with a well defined to moderately well defined border. This finding with other findings is consistent with simple bone cyst. Video 1.
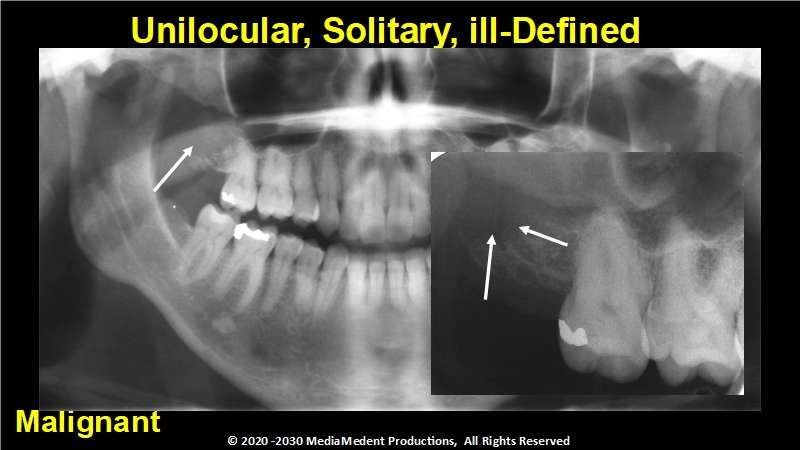
Lecture 5: Radiolucent Lesions Not Associated with Teeth, Unilocular, Solitary, and ill defined Radiolucencies. This ill-defined radiolucent lesion that involved the maxillary right tuberosity was ultimately found to be malignant with histologic characteristics of metastatic disease. Video 1.

Lecture 6: Radiolucent Lesions Not Associated with Teeth, Unilocular, Multiple Radiolucencies. These images illustrate a rare case of multiple myeloma diagnosed in a patient only six months old. The images clearly demonstrate the radiographic finding of multiple “punched out” lesions. Video 1.
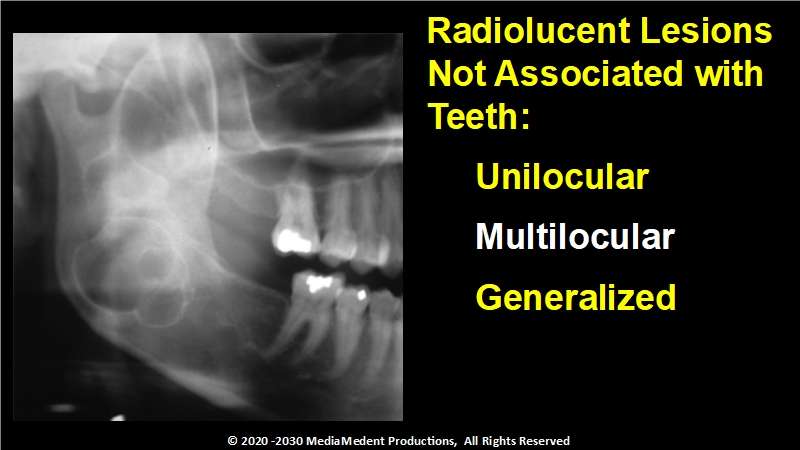
Lecture 7: Radiolucent Lesions Not Associated with Teeth, Multilocular Radiolucencies. Radiolucent lesions may present as unilocular, having a single pathologic compartment, multilocular as in this case containing two or more pathologic chambers partially separated by septa of bone, or generalized radiolucencies. Video 1.
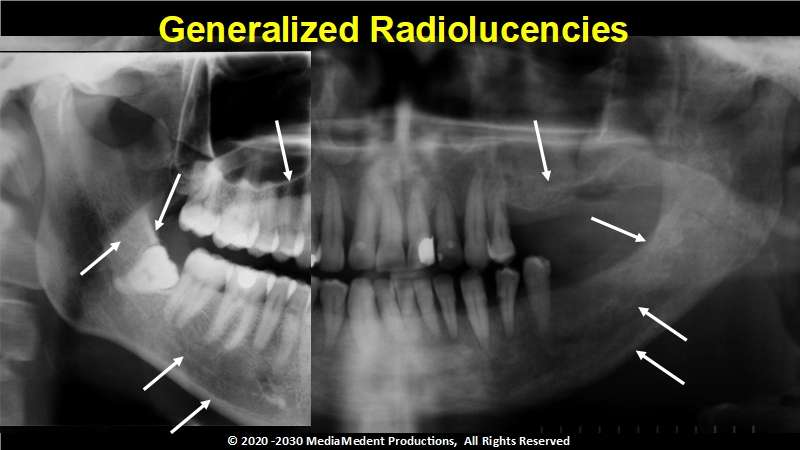
Lecture 8: Radiolucent Lesions Not Associated with Teeth, Generalized Radiolucencies. Compared to the image on the left to that on your right the walls of the maxillary sinus appear less distinct and while the inferior alveolar canal may be located by its radiolucent appearance, there is no cortication of its walls. These findings are consistent with a lesion presenting with a generalized radiolucent appearance. Video 1.
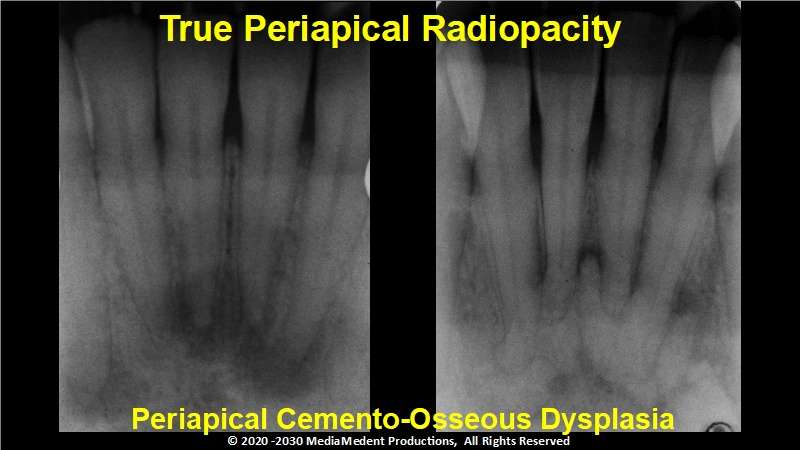
Lecture 9: Radiopaque Lesions Associated/Superimposed with Teeth. As periapical cemento-osseous dysplasia matures radiopaque tissue appears within the radiolucent structure giving the lesion a mixed, radiolucent/radiopaque appearance. In the last stage the lesion is almost completely radiopaque usually with a thin radiolucent margin. Video 2.
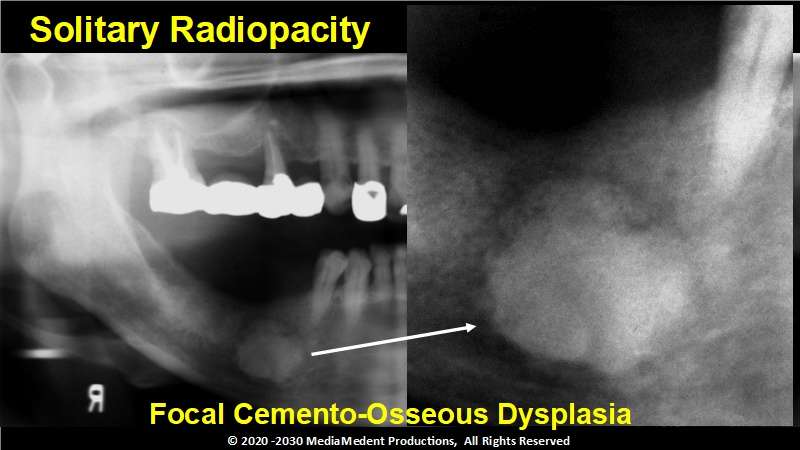
Lecture 10: Radiopaque Lesions Not Associated with Teeth, Solitary Radiopacities. Focal cemento-osseous dysplasia demonstrates single site involvement. While they may occur in any area of the jaws the posterior mandible is the predominant site. Like all cemento-osseous dysplasia’s, focal cemento-osseous dysplasia begins as a radiolucency, matures into a mixed radiolucent/radiopaque stage, and ultimately becomes mostly radiopaque. Video 2.
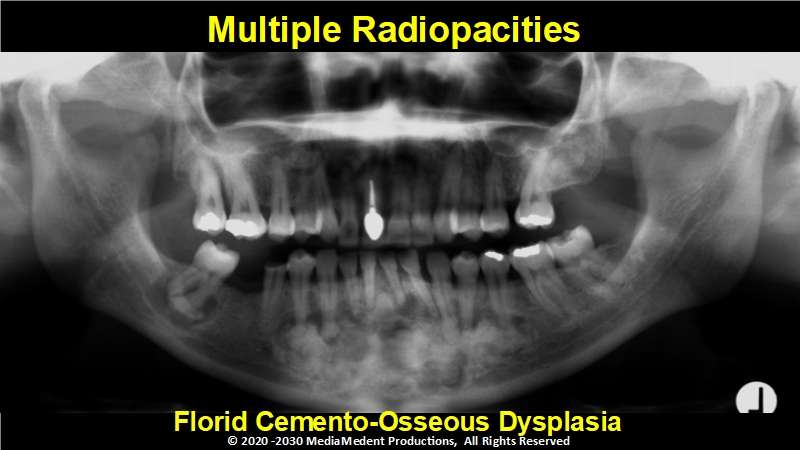
Lecture 11: Radiopaque Lesions Not Associated with Teeth, Multiple and Generalized Radiopacities. Florid cemento-osseous dysplasia demonstrates multiple site involvement. The majority of patients affected by florid osseous-dysplasia are black or Asian females in their early forties. The disease is usually occult and found only on radiographic examination. Video 2.
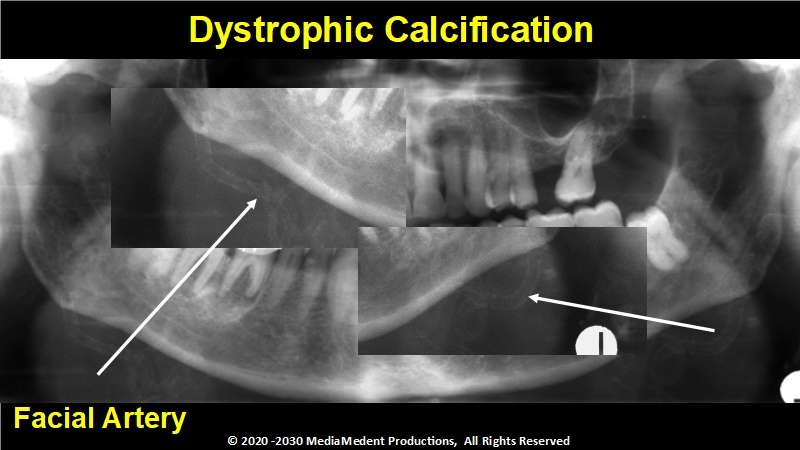
Lecture 12: Radiopaque Lesions, Dystrophic Calcifications. Arteriosclerosis results from the deposition of calcium within the medial coat of vessels. Finding an object with a tube, worm or train track appearance with parallel radiopaque walls and a radiolucent core located in the area of the inferior border of the mandible in the molar region is diagnostic for arteriosclerosis of the facial artery. Video 2.
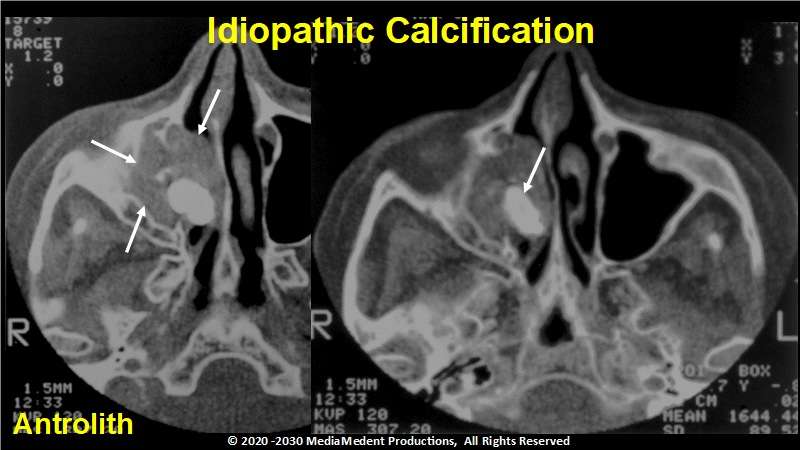
Lecture 13: Radiopaque Lesions, Idiopathic Calcifications, Heterotopic bone, and Foreign Bodies. During the course of the examination a patient related that he experienced chronic sinus congestion on the right side. A panoramic radiograph revealed an irregularly shaped radiopacity of heterogeneous radiodensity within the image of the right orbit. A CT study determined that the radiopacity was an antrolith within the maxillary sinus. Video 2.
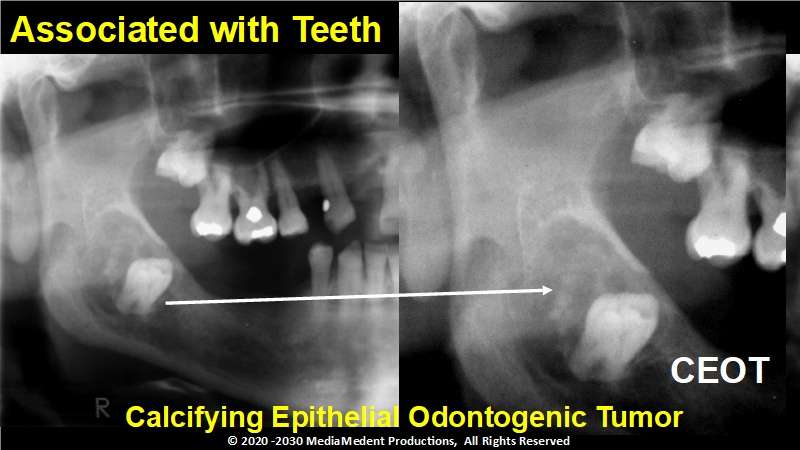
Lecture 14: Radiolucent/Radiopaque Lesions, Associated with Teeth. The calcifying epithelial odontogenic tumor or Pindborg tumor or CEOT is rare, representing only 1 percent of odontogenic tumors. The most common radiographic picture is that of a pericoronal radiolucency with diffuse radiopacities. Video 2.

Lecture 15: Radiolucent/Radiopaque Lesions, Not Associated with Teeth. This example of an osteosarcoma shows the classic sunburst, sunray, or hair-on-end appearance. While it is easy to associate this appearance with the osteogenic sarcoma it should be kept in mind that this is observed in only about 25 percent of cases. Also evident in this example is a widening of the periodontal ligament space around the second molar. Video 2.
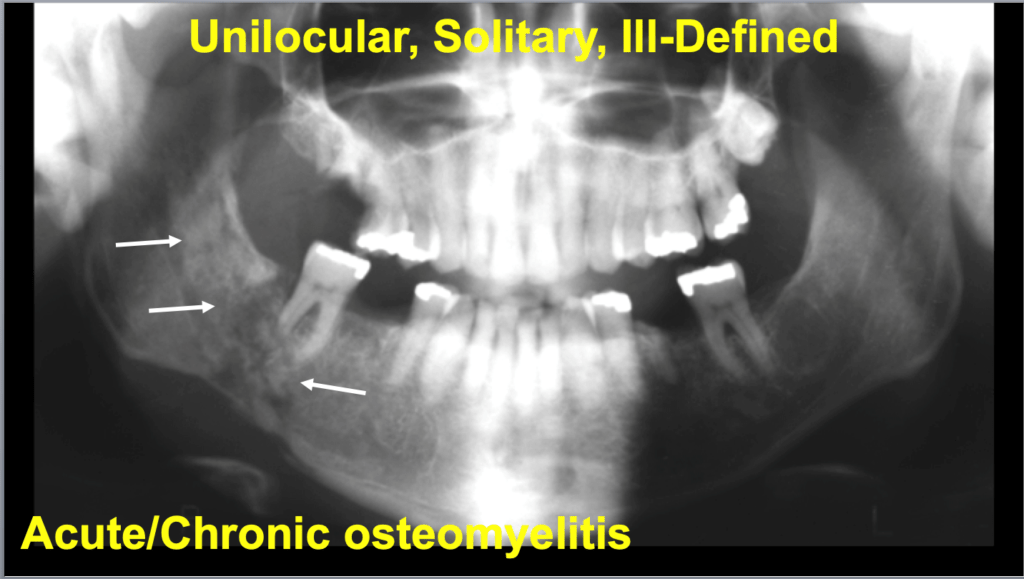
Lecture 16: Comprehensive Self Study Review. Osteomyelitis may affect patients of all ages. There is a predilection for males and it is more commonly found in the mandibular posterior. Typical signs and symptoms of acute osteomyelitis include, but are not limited to rapid onset, pain, swelling, fever, lymphadenopathy, and leukocytosis. Purulent drainage may also be present. Video 2.
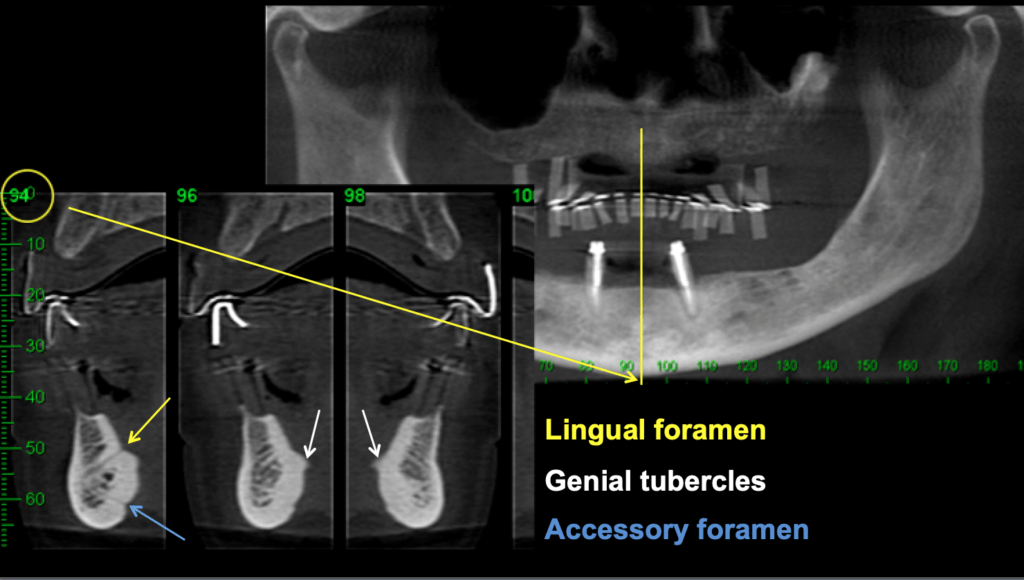
Lecture 17: Review of Intra- and Extraoral Radiographic Landmarks.This lecture is a review of anatomic landmarks found in intraoral, panoramic, cone beam computed tomography, and other extraoral radiographic images. Video 2.